
Local government health capacity and Nepal's Covid-19 response
Key Insights
- Nepali local governments with relatively higher Covid-induced health burdens—measured by Covid-19 caseloads, number of returnee migrants, and quarantine center overload—do not report higher rates of testing and tracing.
- By contrast, health capacity is positively correlated with local governments’ testing and tracing activities. Health capacity is measured by a standardized health index capturing nine indicators on health staff, infrastructure and planning capacities.
Background
Central to Covid-19 response strategy are government actions to contain and mitigate the spread of the disease. These public health actions are ratified by Nepal’s 2015 Constitution as a shared responsibility between different
spheres of government. While primary healthcare and sanitation are exclusive functions of local governments,
recent executive orders have made local and provincial governments responsible for coordinating Covid-19 public health activities. This includes coordination by local governments with provinces for identifying suspected
cases, arranging transportation to swab collection centres, and mobilizing case investigation and contact tracing teams.
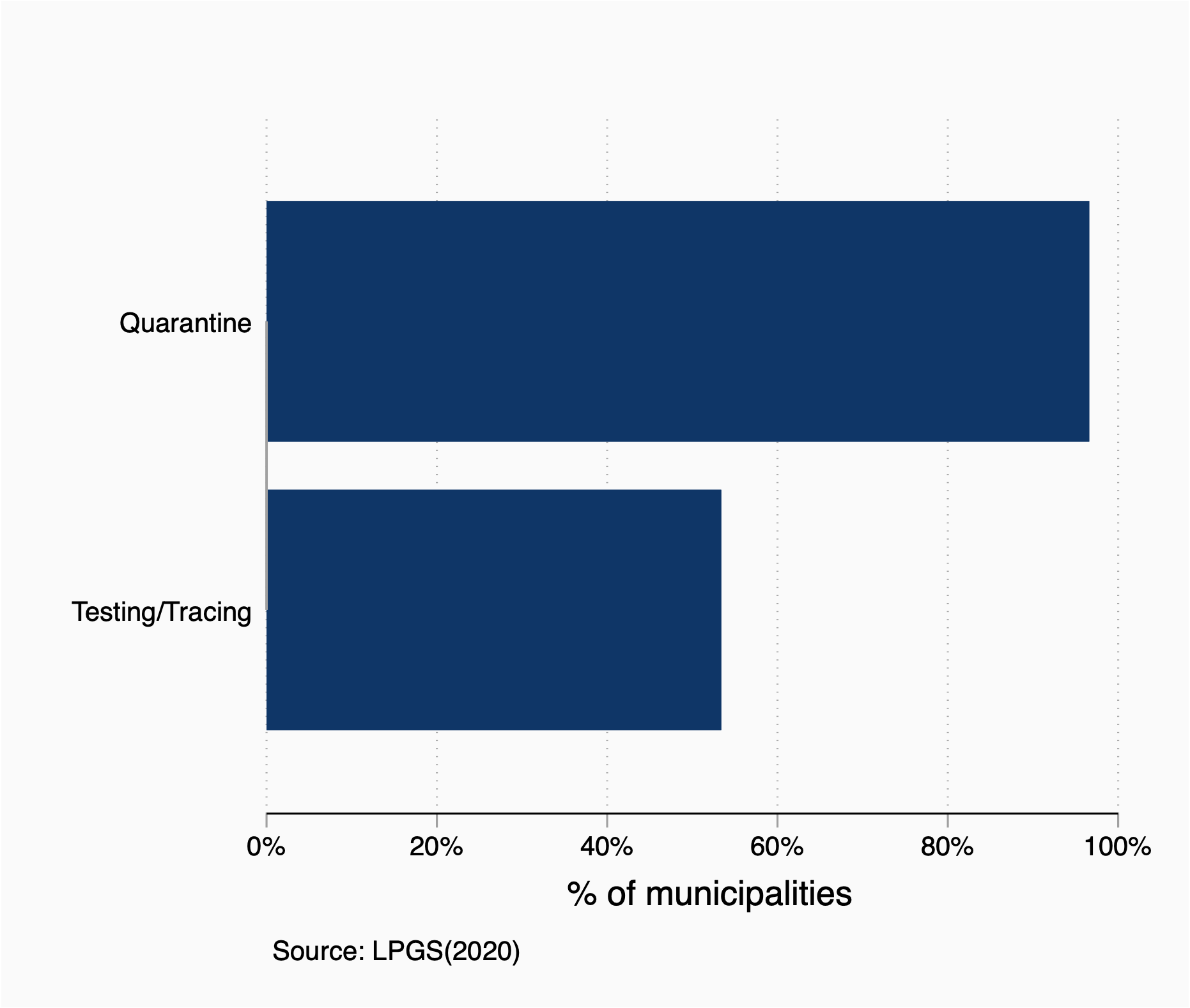
Researchers from Yale University, London School of Economics, Governance Lab (Kathmandu) and Nepal Administrative Staff College (NASC) carried out the Local and Provincial Government Survey (LPGS) on Covid response from a nationally representative sample of 113 local governments in June 2020. This survey provides an analysis of testing and tracing activites reported by local governments. In contrast to universal (97%) local government involvement in set-up and management of quarantine and holding centres, only 53% local governments reported supporting testing of potential cases and contact tracing (Figure 1).
To understand the variation in testing and tracing activities by local governments, we consider two factors. First, municipality Covid burden measured by Covid cases at district level, number of returnee migrants, and quarantine center overload. Second, local government health capacity measured by a health index using the data from the Federalism Capacity Needs Assessment (FCNA) survey and the Health Management Information System (HMIS). The health index (see box below) includes indicators for staff shortage, particularly health related staff, number of hospitals in municipalities, and planning and monitoring capacities of local government in health sector.
Key Findings
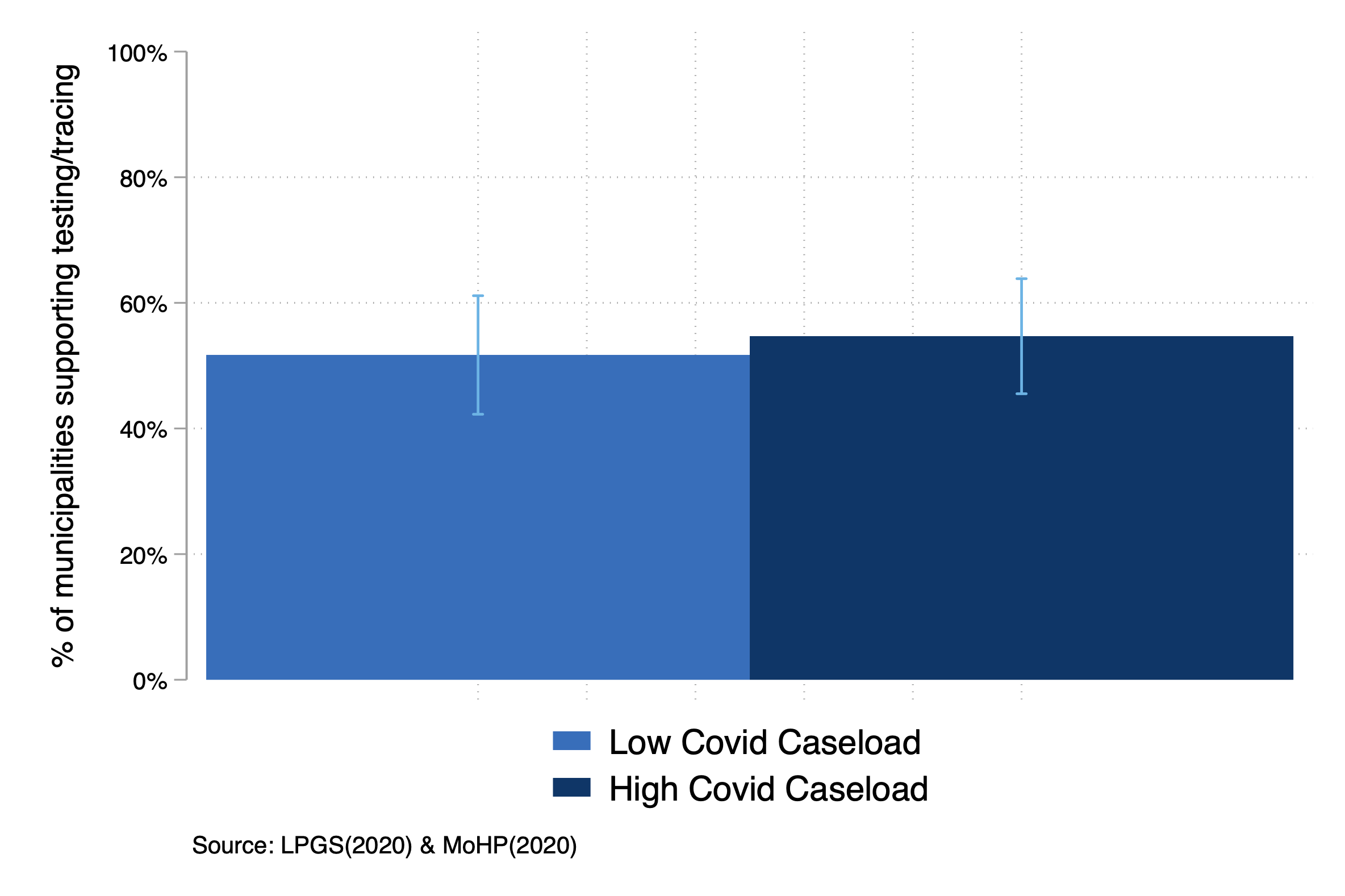
Finding 1: Testing and tracing activities do not vary by municipality Covid-19 burden.
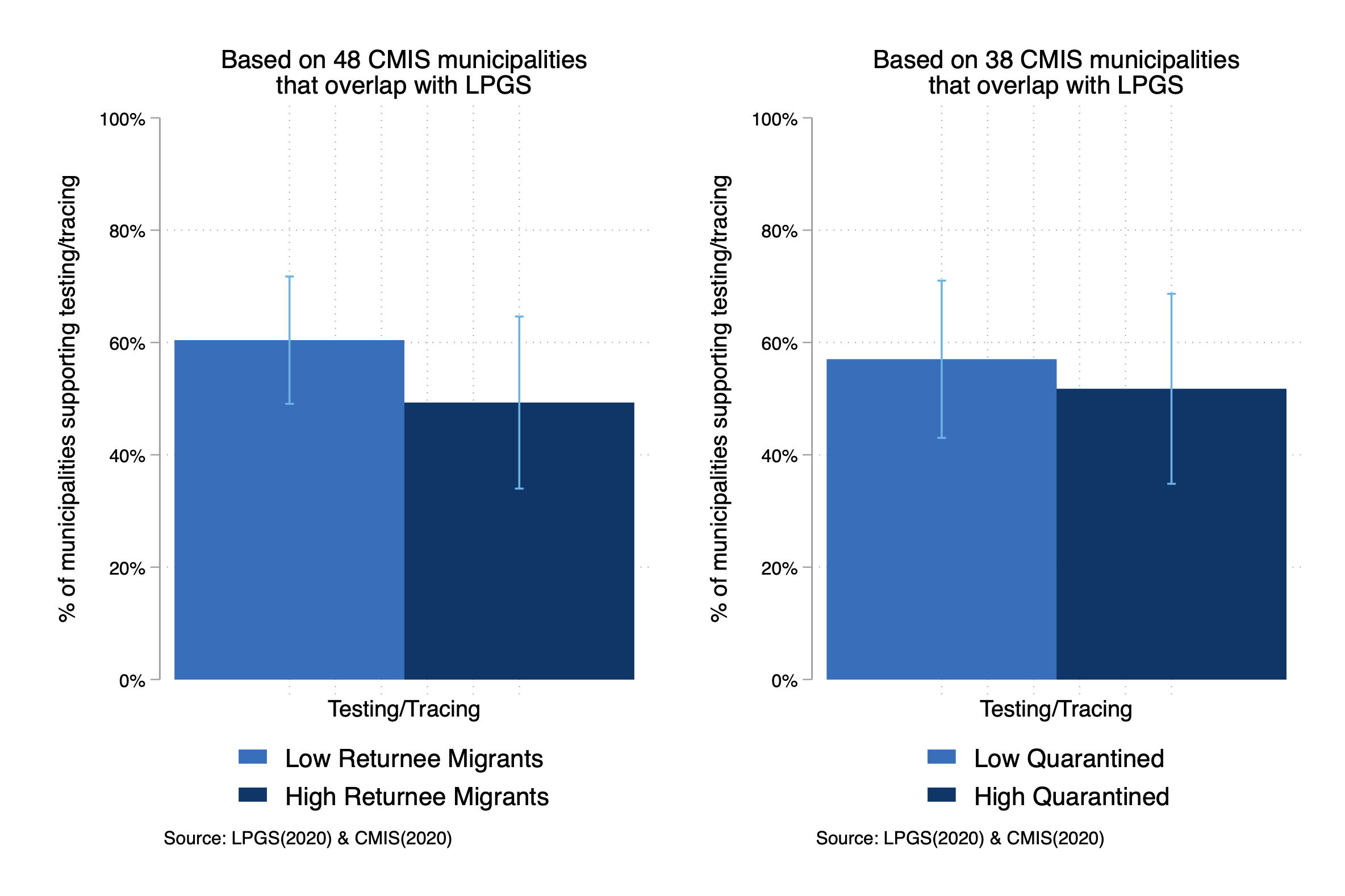
We also used data on returnee migrants and quarantined individuals as alternative indicators of Covid burdens. Although these are from a limited number of local governments that reported into the Ministry of Federal Affairs and General Administration (MoFAGA) through the Crisis Management Information System (CMIS), using this data we see the same pattern (Figure 3).
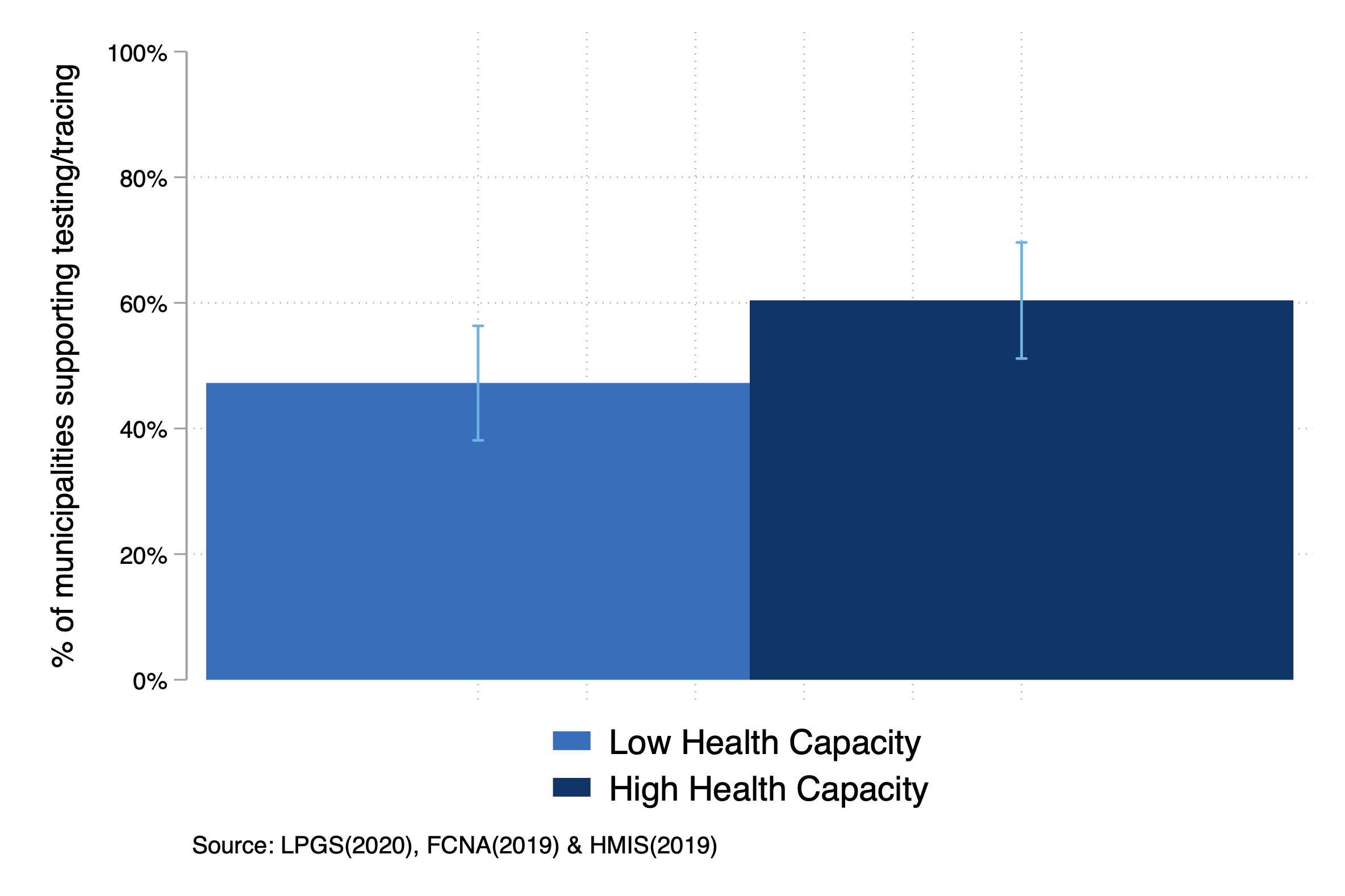
Finding 2: Higher health capacity of local government predicts greater testing and tracing support by them.
Local governments with high health capacities are 13 percentage points more likely to report engaging in support of testing of potential cases and contact tracing activities (Figure 4).
Recommendations
We find that testing and tracing activities by local governments do not vary by COVID-induced burdens but they do correlate with their pre-existing health capacities. Nepal’s policymakers can use existing administrative data to create rankings of health capacity of local governments across Nepal. These rankings can be used for taking Covid-related policy actions by helping to compensate for local governments with poor health infrastructure and staff, or low planning capacity. Not only can these actions assist in checking of the spread of Covid-19 today, they may come in useful in providing the necessary support for distribution of vaccine when it becomes available.
Health Index:
We use Kling Liebman Katz (KLK) index method to generate a health index as a measure of health capacity. This method first standardizes health capacity related variables against their mean and standard deviation and then combines those standardized variables by taking their average to construct the index. The index values are distributed around mean zero. A positive value of this index signifies relatively high health capacity, while a negative value is low capacity. The distribution of the health index across Nepali municipalities is positively skewed.